Breast Intervention BasicsGreat call!
Finding a subtle, subcentimeter area of architectural distortion on a screening mammogram can feel really good. But oftentimes, the sense of accomplishment gives way to a sense of dread as you realize you now have to figure out how to sample this lesion. 
The vast majority of breast biopsies performed today are percutaneous core biopsies. These quick, safe and accurate procedures have nearly completely replaced open surgical biopsies or Fine-Needle Aspirations (FNA). While the procedures are relatively simple, there are a few places where you can get tripped up if you are not paying attention.
Biopsy Needle Options
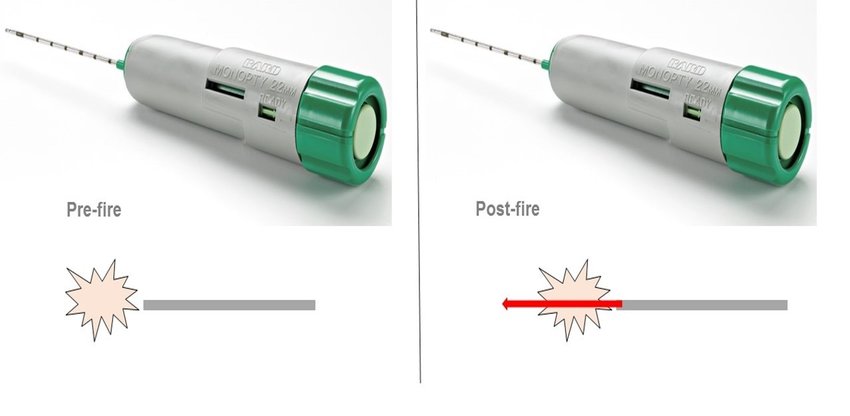
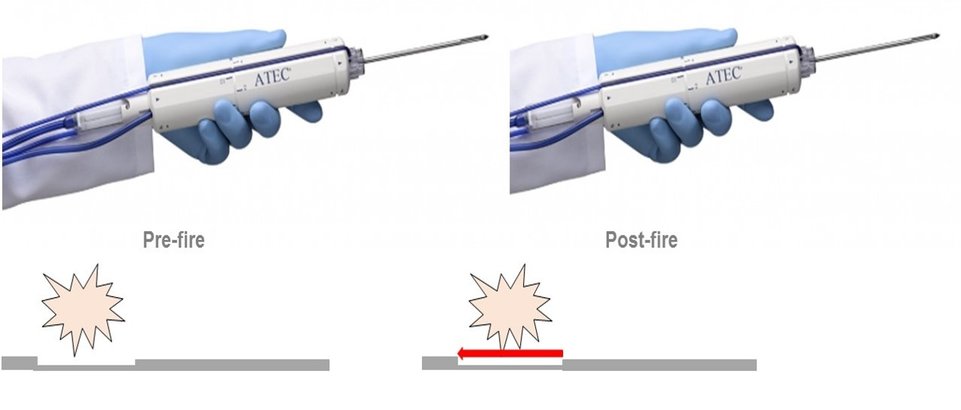
Breast core biopsy needles come in a variety of sizes. Needle size is measured in gauge (thickness) and length. In general, the most common length of biopsy needles are either 10cm or 16cm. The more important measurement is the thickness or gauge of the needle. Smaller gauge = larger outer diameter (bigger needle & more tissue acquired) Larger gauge = smaller outer diameter (smaller needle & less tissue acquired) The most common needle gauges used in the breast vary depending on the type of biopsy. Ultrasound core biopsies typically use a 14g or 12g needle. Stereotactic core biopsies typically use larger needles such as 7g, 9g or 12g. MRI biopsies usually use 9g or 12g needles as well. Type of Breast Biopsy Guidance
Core biopsies of the breast can be performed using ultrasound, mammographic, or MRI guidance. In general, the modality on which you can see the lesion best is the optimal way to perform the procedure. That being said, ultrasound core biopsies are the quickest and most cost effective type of breast intervention and should be your first choice if at all possible. 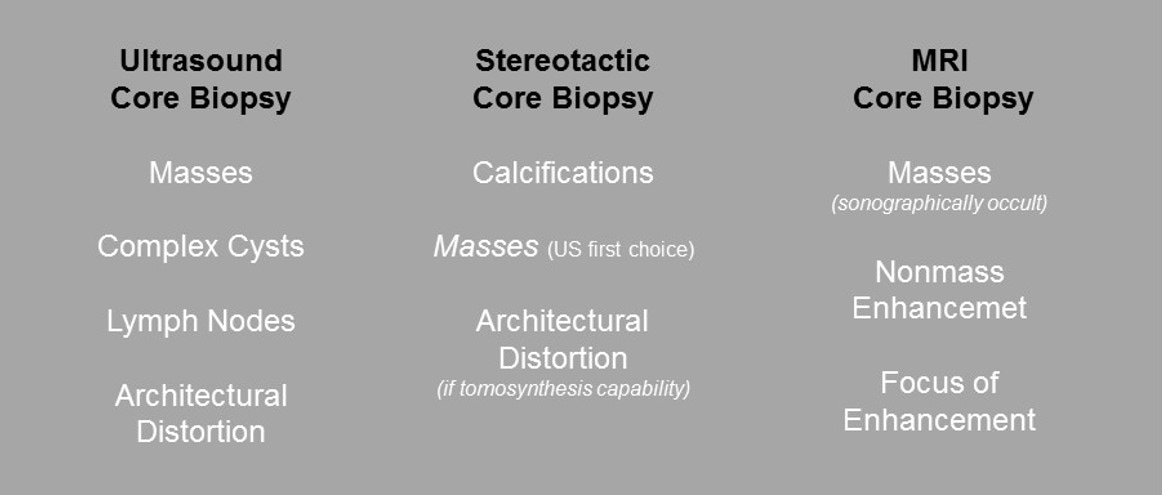
Figure 1. Best Way to Biopsy Specific Breast Lesions
|
|