|
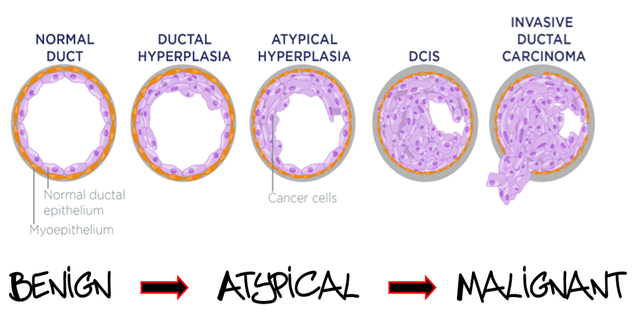
Anytime you perform a breast biopsy there are three possible outcomes.
The result may come back completely benign, in which nothing further needs to be done. Alternatively, on the other end of spectrum, the biopsy may reveal malignancy. Both of these outcomes are fairly straightforward. When you do a biopsy, occasionally you will get a third outcome. The result will be Atypical. Meaning, not normal yet not breast cancer. There are many pathologic entities that fall into this Atypical or High Risk bucket. |
|
|
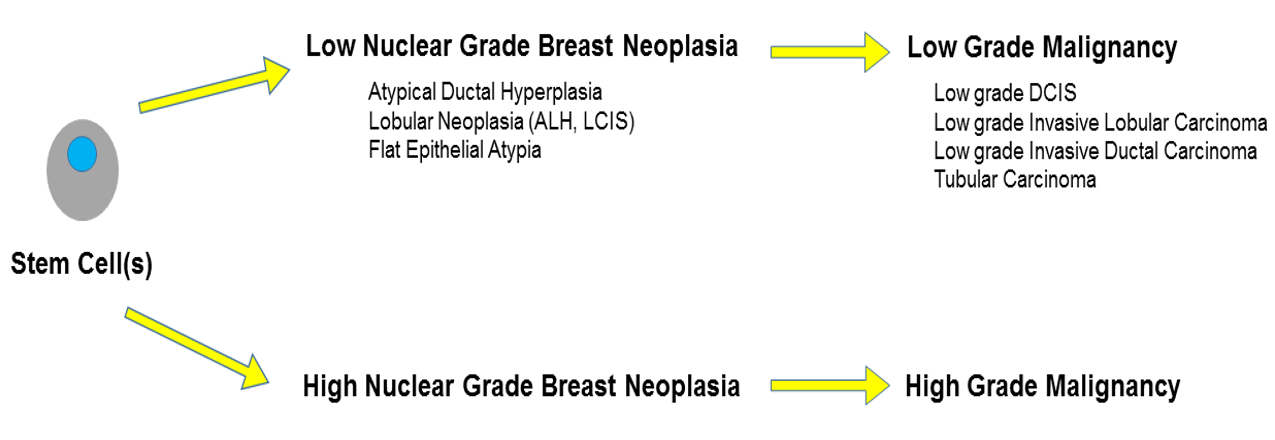
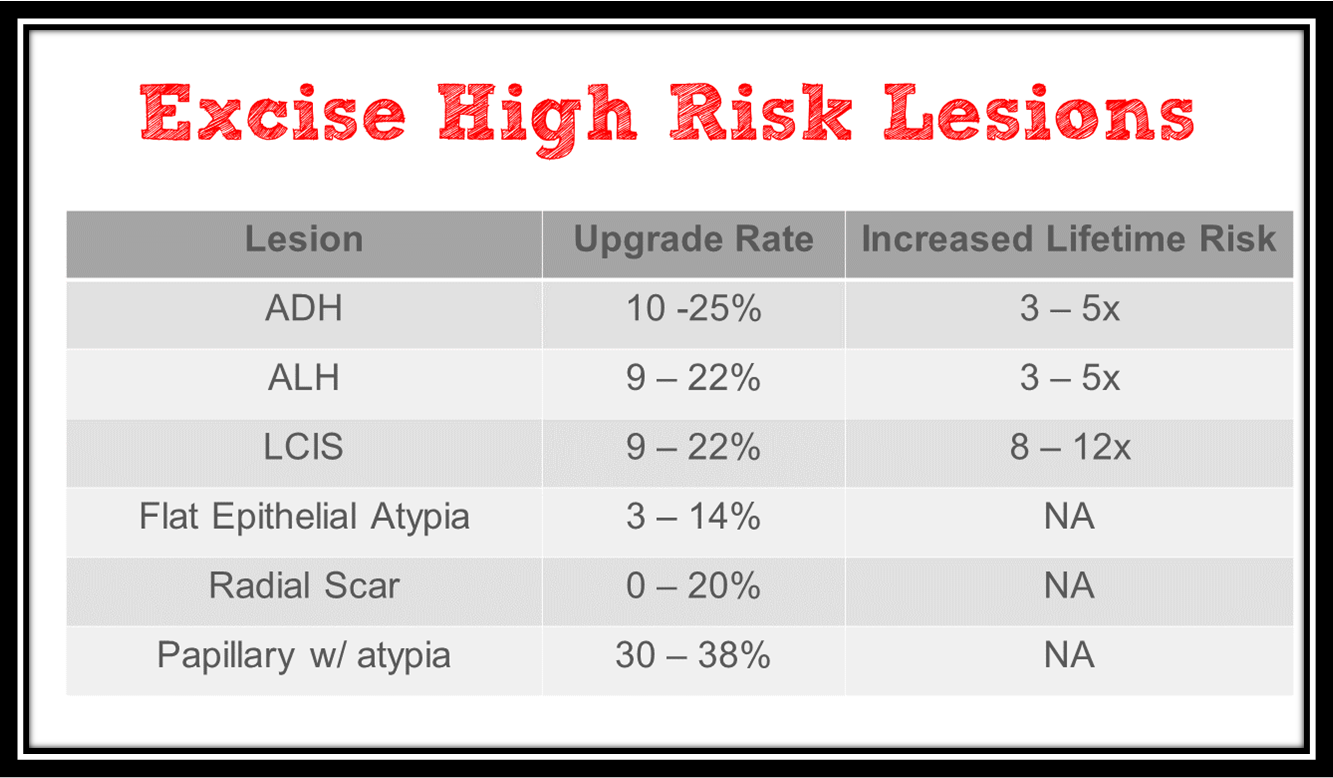
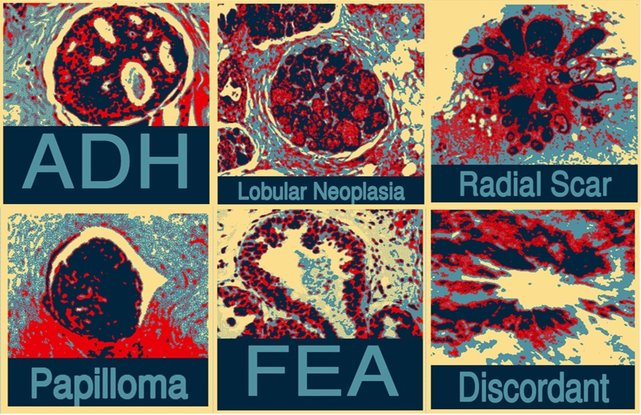
Atypical Ductal Hyperplasia (ADH)
Increased layers of "funky" looking epithelial cells in the TDLU (Terminal Duct Lobular Unit). Has a significant upgrade rate. Increases ones lifetime risk of breast cancer. Atypical Lobular Hyperplasia (ALH) Categorized as Lobular Neoplasia, small discohesive cells may be found incidentally at biopsy. Partial involvement of the lobule. Has a significant upgrade rate. Increases ones lifetime risk of breast cancer (bilaterally). Lobular Carcinoma In-Situ (LCIS) Categorized as Lobular Neoplasia, small discohesive cells may be found incidentally at biopsy. > 1/2 of the lobule is involved. Has a significant upgrade rate. Increases ones lifetime risk of breast cancer (bilaterally). Pleomorphic LCIS Categorized as Lobular Neoplasia, more aggressive subtype that is often strongly Her2+. Very high upgrade rate. Increases ones lifetime risk of breast cancer, but also has a high rate of recurrence. Flat Epithelial Atypia (FEA) Also known as columnar cell change with atypia. Low grade cytologic atypia, frequently found incidentally at biopsy. Has a low upgrade rate (but often found in presence of other high risk lesions). Slight increase in ones lifetime risk of breast cancer. Radial Scar / Complex Sclerosing Lesion Stellate lesion with a central elastotic core, maintains myoepithelial layer. Variable upgrade rate. Minimal, if any increase in lifetime risk of breast cancer. Occasionally, co-existing malignancy. Intraductal Papilloma +/- Atypia Benign intraductal proliferation with a fibrovascular core. Controversial if need to remove every intraductal papilloma (? only remove if > 1.5 cm in size). All papillary lesions with atypia need to be removed. Variable upgrade rate (essentially zero if no atypia) due to undersampling & heterogeneity. |
|
Phyllodes Tumor (also referred to as a fibroepithelial tumor with cellular stroma) Difficult to distinguish from the common benign fibroadenoma with a cellular stroma. Most are benign but can grow quickly and to a very large size. 1 out of 10 is a malignant Phyllodes (acts and treated more like a sarcoma). High rate of local recurrence so excision with wide margins recommended. Mucocele-Like Lesions Mucin within the breast stroma, usually due to a ruptured duct. Significant risk of underdiagnosis & difficult to distinguish from mucinous carcinoma. Fibromatosis (extra-abdominal Desmoid) and Nodular Fasciitis Locally aggressive stromal tumors. No risk of metastasis. Require wide excision to prevent recurrence. Granular Cell Tumor Rare neoplastic growth from peripheral nerve Schwann cells. Usually benign, but occasionally co-existing malignancy. Any other Atypia (ex. Atypical Apocrine Metaplasia) Variable upgrade rates. Diagnosis may change to ADH, ALH or LCIS at surgical excision. |
|
The breast procedures section of our Master Breast Imaging training program is second to none.
Packed with in-depth, step by step instructions for performing ultrasound guided, stereotactic and MRI guided biopsies. Wire localizations and aspirations are also covered. Multiple challenging scenarios are covered such as small breasts, implants, one view findings and more. We feel confident saying this course is unlike any other on the market. |