
|
|
|
|
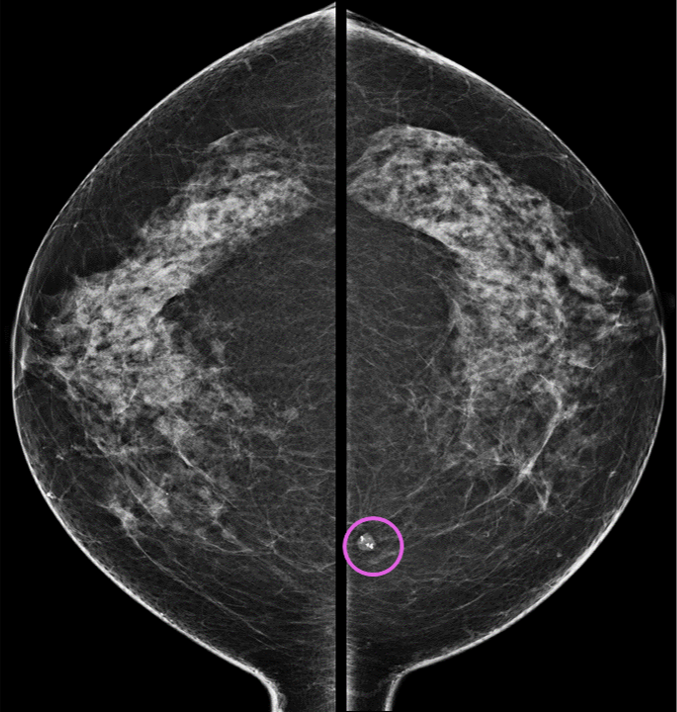
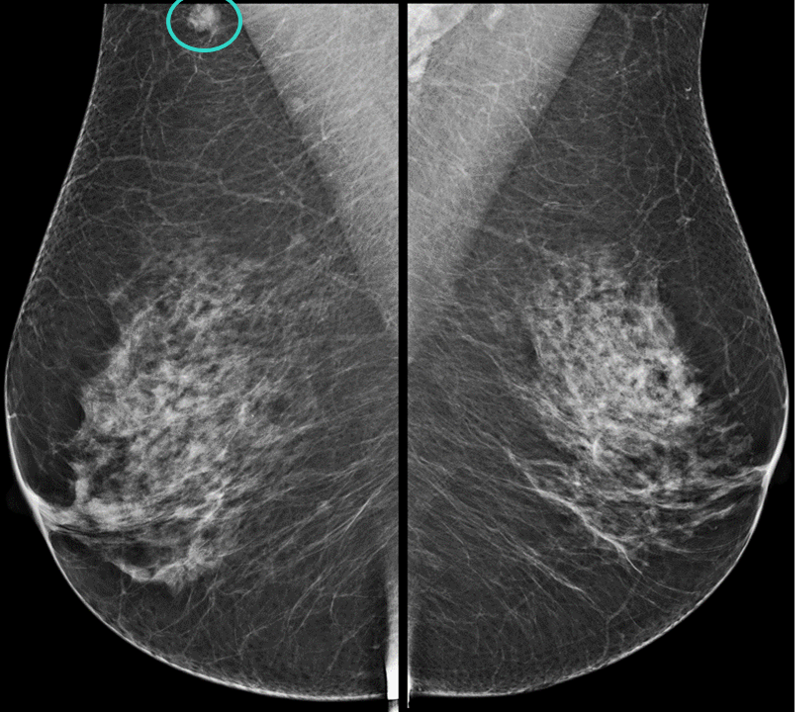
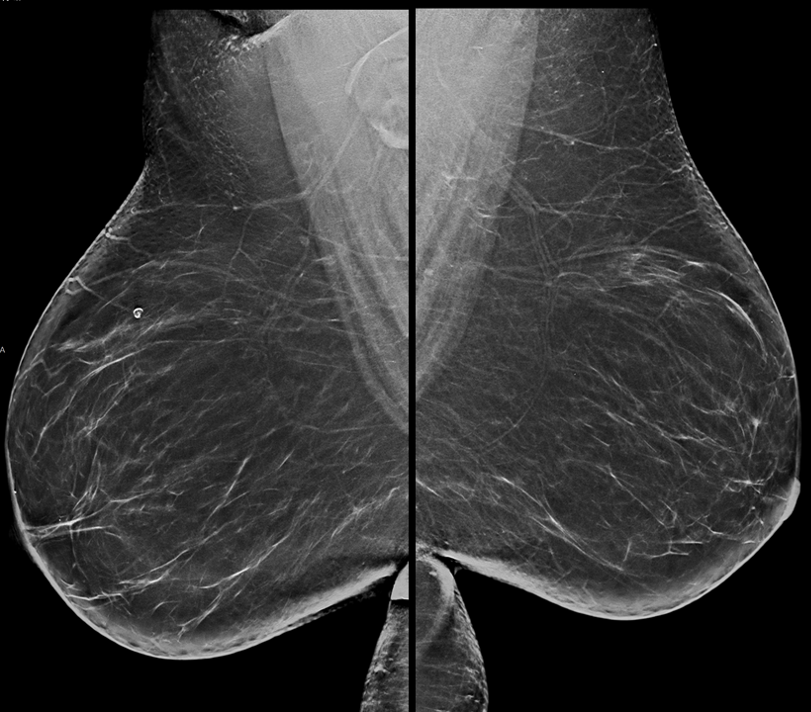
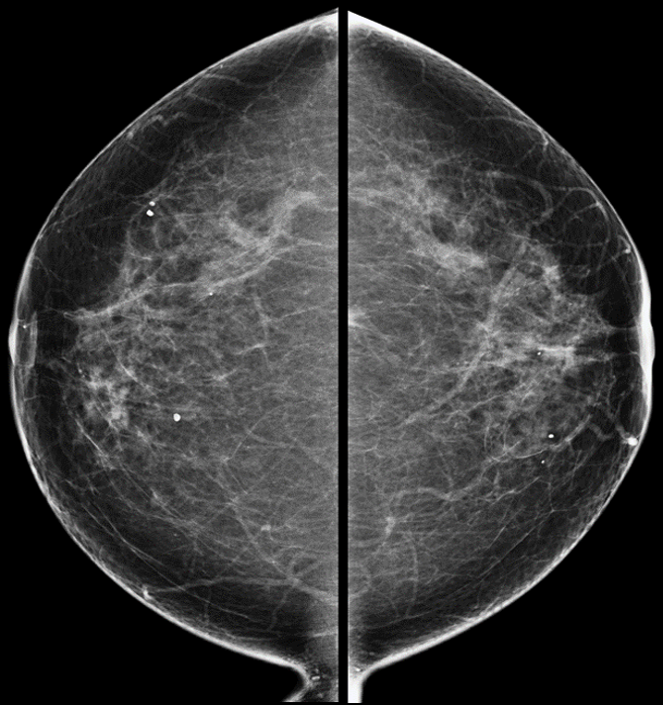
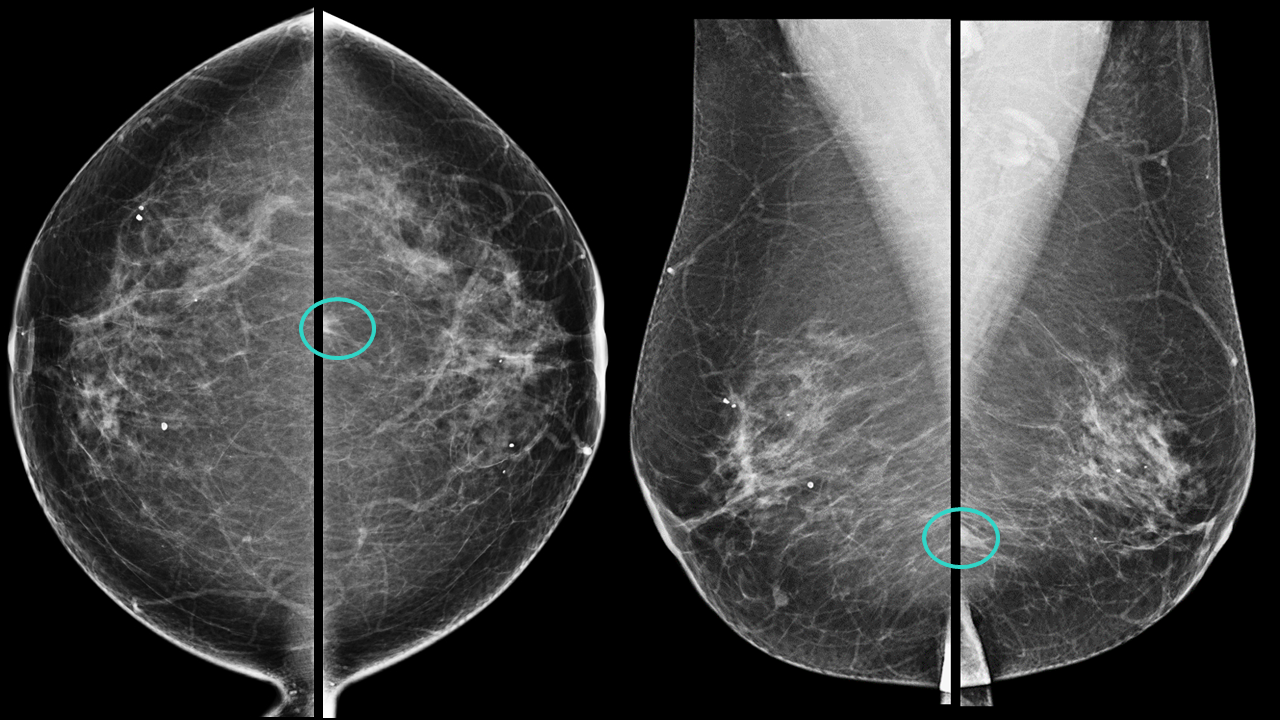
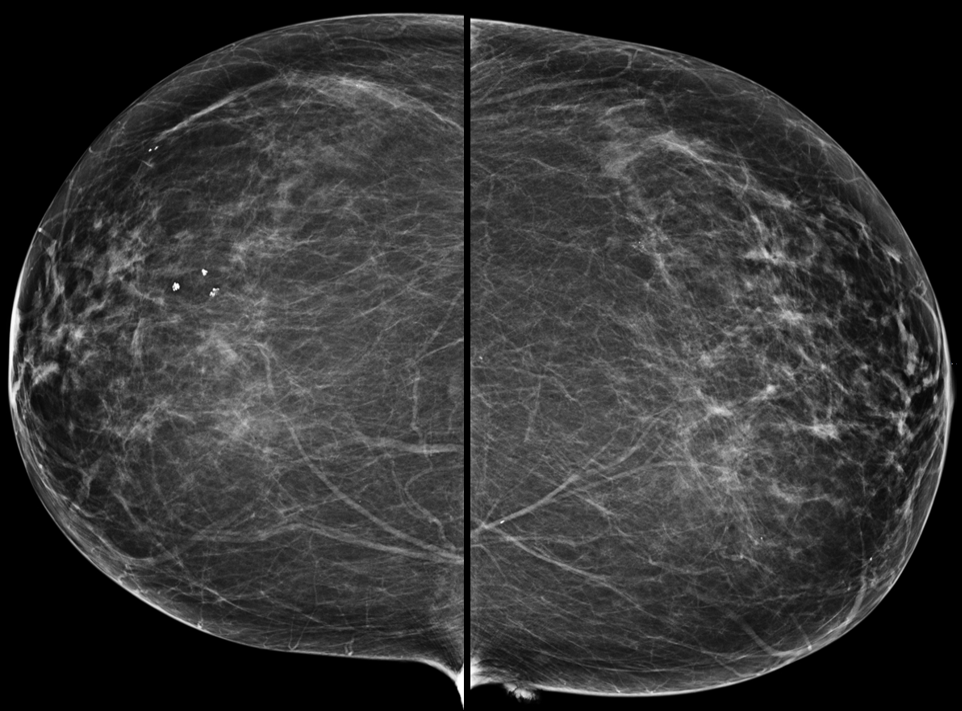
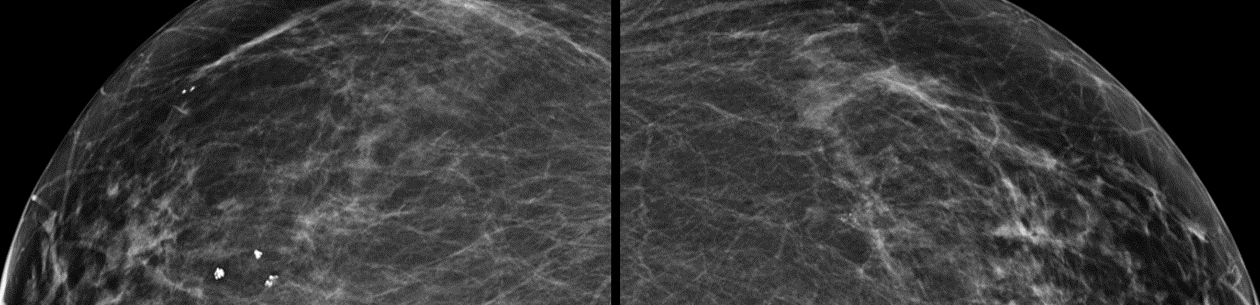
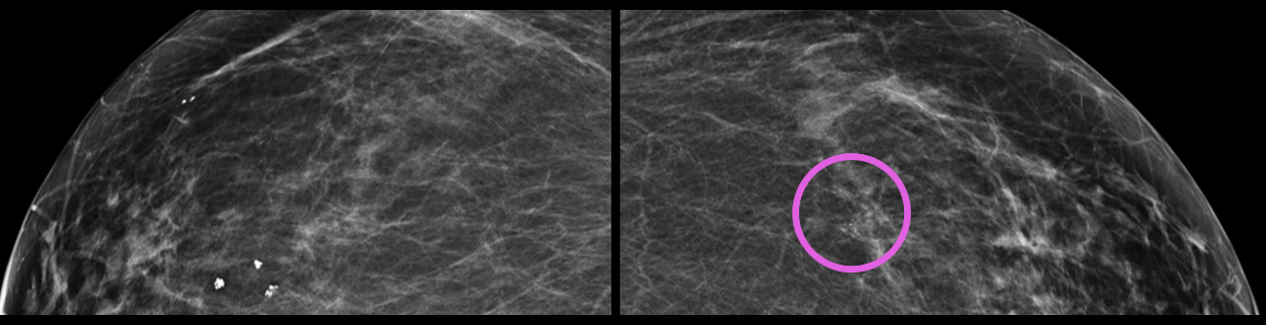
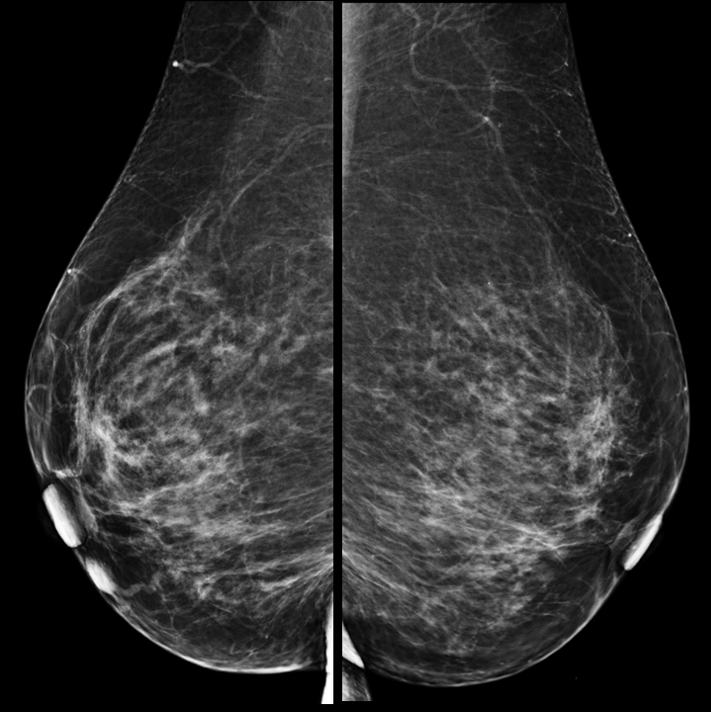
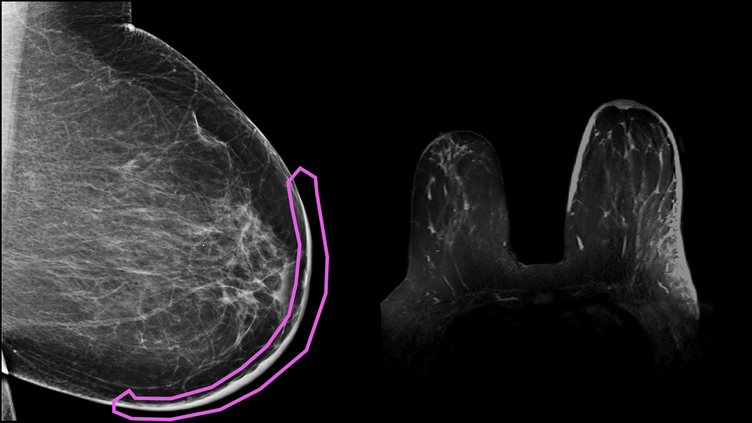
Mass in the axillary region of the right breast requires further evaluation.
|
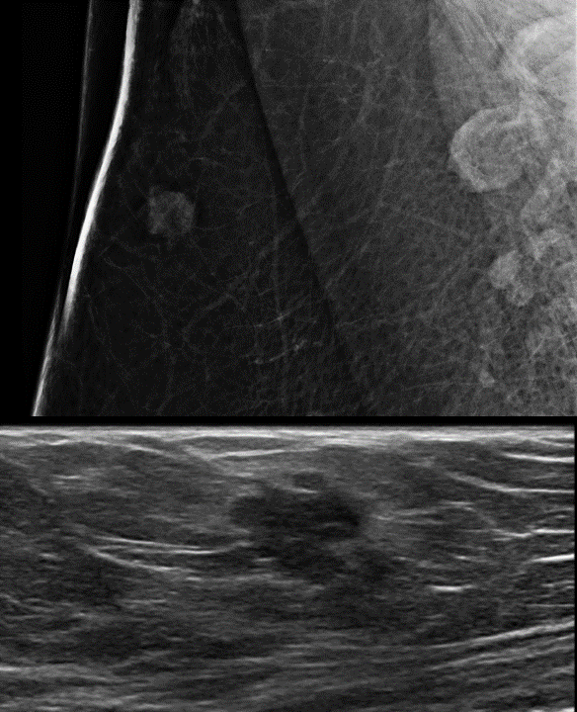
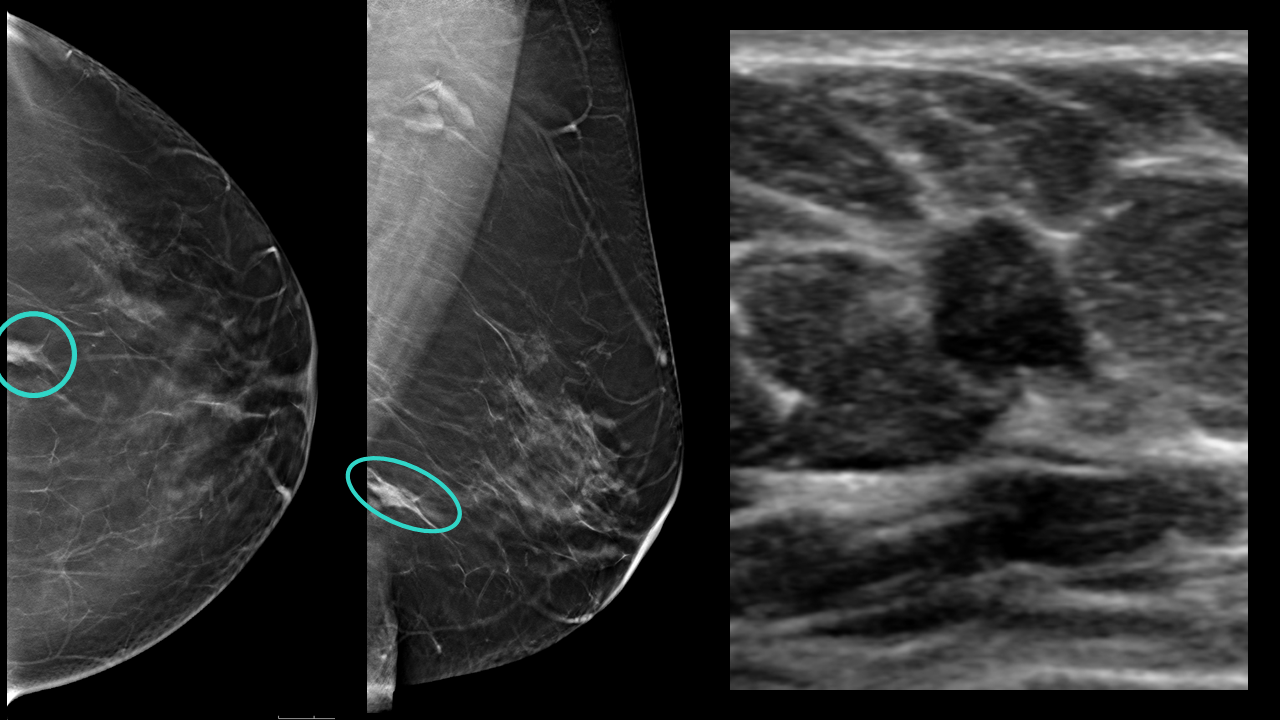
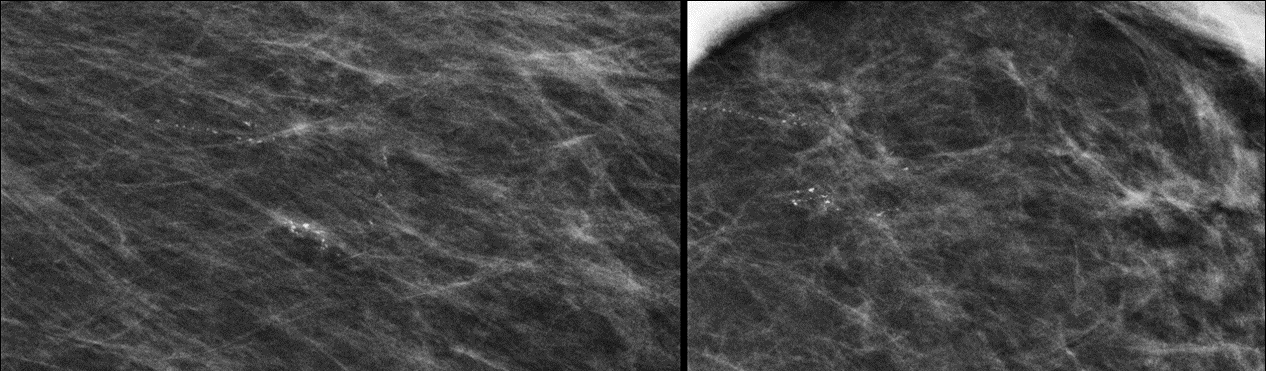
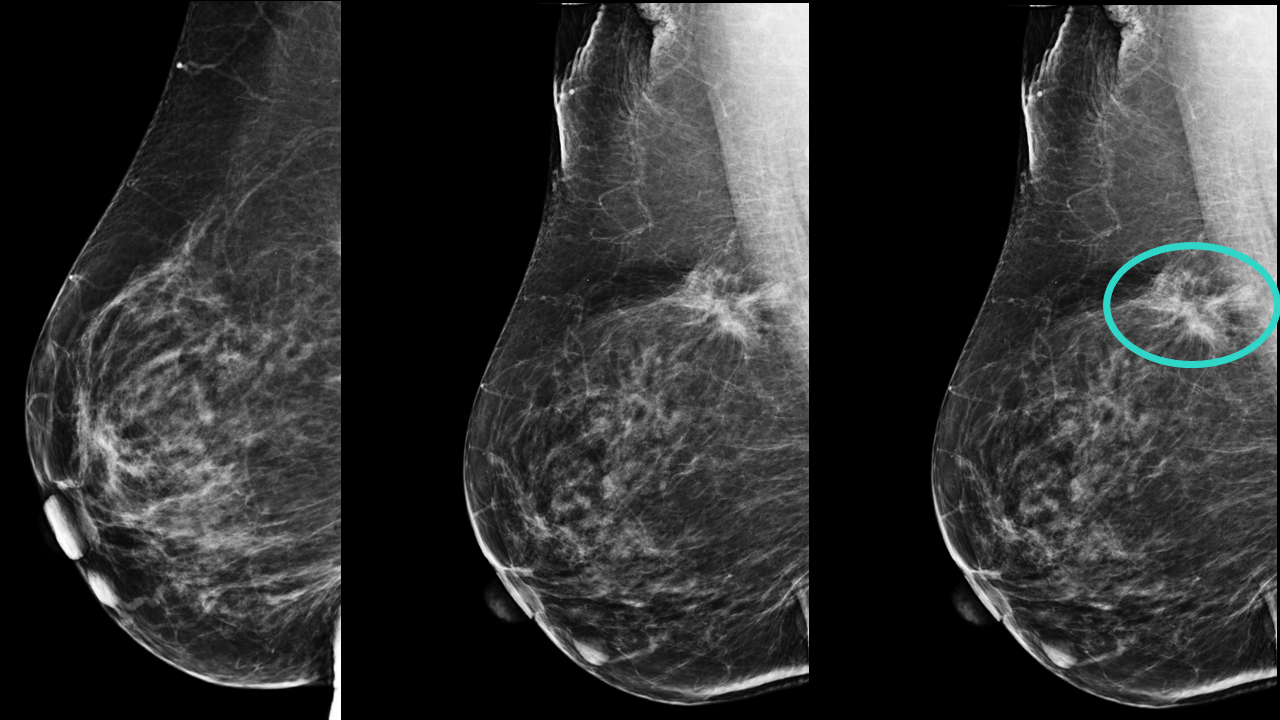
Spot magnification view and an ultrasound demonstrates a spiculated mass in the axillary tail of the right breast.
|
|
|
|
|
|
|

|
|

|
Good breast ultrasound images allow for more specific diagnoses, limit misdiagnoses, and in general are more actionable.
Some features of high quality ultrasound exams include:
|
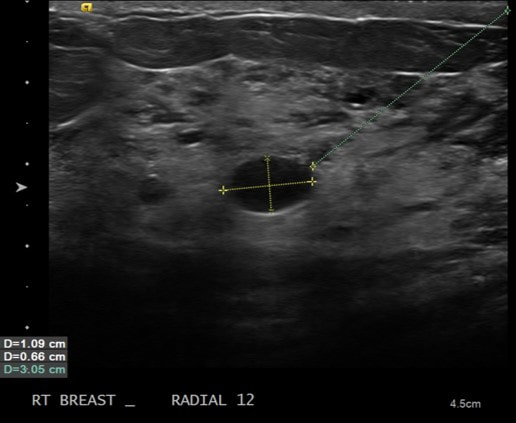
Avoid unnecessary and inaccurate measurements. All they do is waste time and confuse people.
|
When you make a finding (mass, cyst, etc), appropriate labeling of the location requires the clock position and approximate distance from the nipple.
Please note the word approximate. No need to measure the distance from the nipple or depth of a lesion with calipers. This is totally inaccurate. If the patient rolls on their side or shifts position, the measurement and certainly the lesion depth will change. Save time and just estimate the distance between your probe and the nipple to the nearest centimeter. Also, please avoid measuring all cysts in 2 or 3 dimensions. It is meaningless. Cysts fluctuate in size over time (due to hormone changes, medications, caffeine, other external factors). If you measure the same cyst 2 weeks later it will be a different size (or maybe even resolved and no longer present). Don't waste your time. |

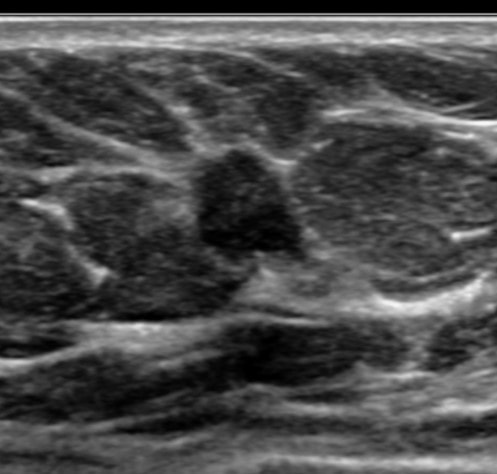
If you adjust the gain and brighten the image to more appropriate levels, this is an obvious suspicious solid mass.
|
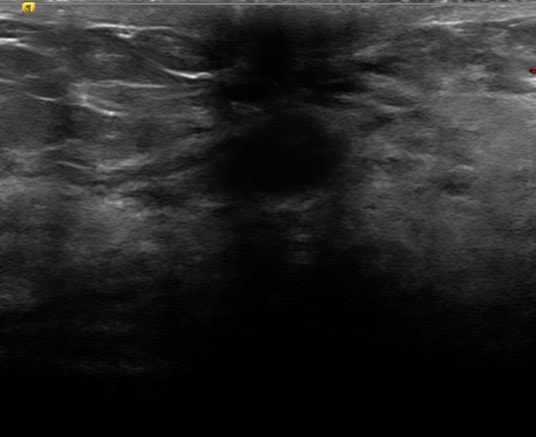
Big simple cyst, no big deal. Next case.
Wrong! This is a large grade 3 triple negative invasive ductal carcinoma. The problem here is inappropriate gain. The ultrasound is only as good as the operator. With the twist of a few knobs, you can make any solid mass appear cystic. DON'T DO THIS! Ensure that the gain is appropriate on all exams. A good way to gauge is to ensure that the background fat is isoechoic (gray) and not anechoic (black) as in this case. |
A lesion is present underneath the nipple, however poor technique limits even the most basic assessment as to if it is cystic or solid.
|
Diagnosis please??
If you hesitated, I don't blame you. How in the world can you tell what this is? You can't, the images are non-diagnostic. Clearly, there is some sort of mass or cyst underneath the nipple. But one is not able to say much more than that about it. And what happened to the pec muscle. There are several special techniques that can be used when imaging near the nipple-areolar complex that would have fixed this image. The frightening and discouraging thing is what the report stated on this case. "Lesion in the subareolar left breast. MRI is recommended to evaluate." Poor technique and lazy interpretation made this a wasted exam. |
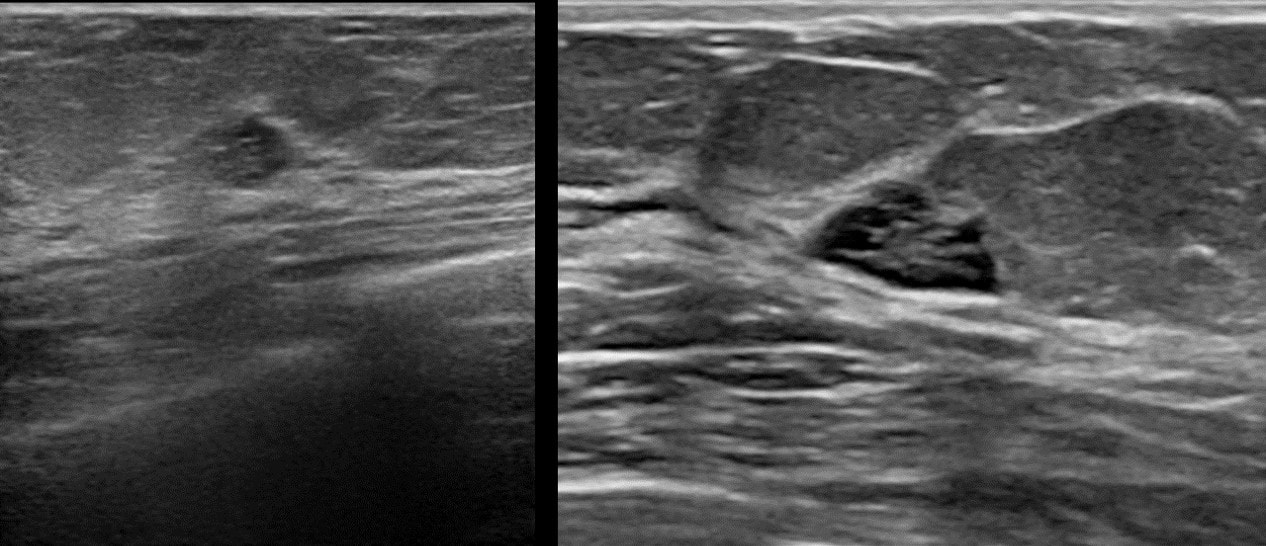
Two ultrasound images of the same mass performed 2 days apart. Notice the dramatic difference in image quality.
|
Using the right equipment and appropriate technique is essential when performing breast ultrasound. Look at the difference in image quality and how the image on the right clearly shows a complex cyst. The next step is then automatic, a biopsy is required.
However, if given only the first low quality image on the left, it becomes much more difficult to make a definitive diagnosis and actionable next step. |

|
|
|
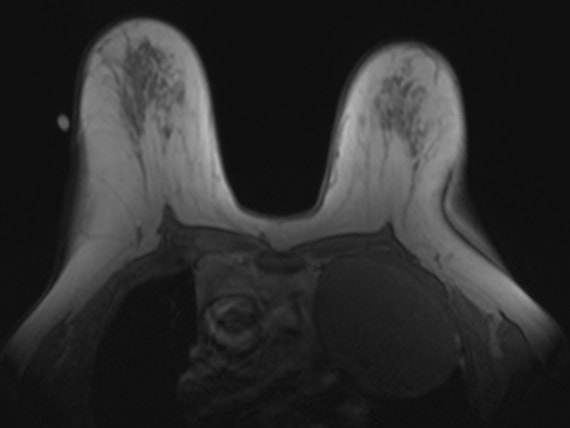
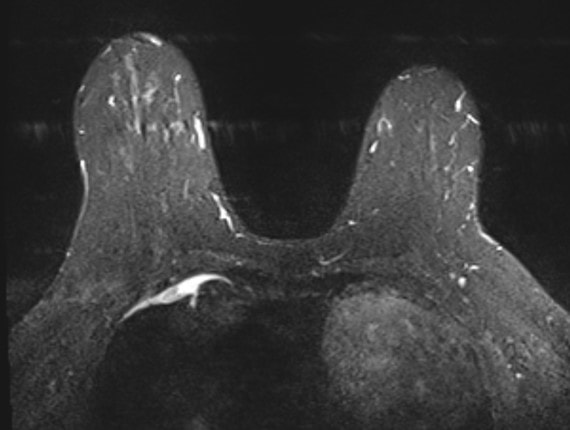
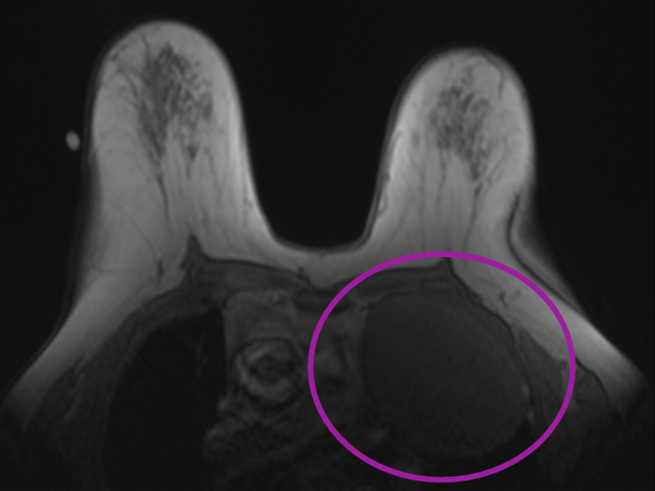
Even though the exam is designed to image the breasts, a large part of the neck base, chest and upper abdomen are often included in the images.
You are responsible for any major findings. The patient in case 1 had an incidentally detected solitary fibrous tumor of the pleura which was subsequently excised. Typically, the most useful sequences to evaluate the "non-breast" structures tend to be the STIR and any non-fat saturated T1 images. |

|
|

|
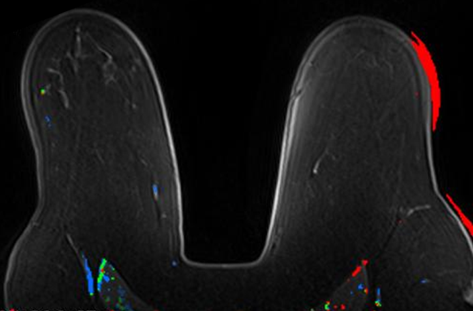
Suspicious enhancing mass in the lower outer quadrant of the left breast.
|
Remember, each sequence on a MRI exam has a unique purpose. Don't just blindly scroll through every sequence.
The MIP is to get an overview, on post-contrast images you are looking for enhancement, on the STIR images for T2 hyperintense lesions in the breast or elsewhere in the body. Once you find a mass, determine whether it enhances. If so, what is the kinetic profile? Is it T2 bright? Does it contain fat on the non-fat saturated T1 sequence? You are a detective, use each breast MRI sequence as a tool to help solve the mystery. |
|
|
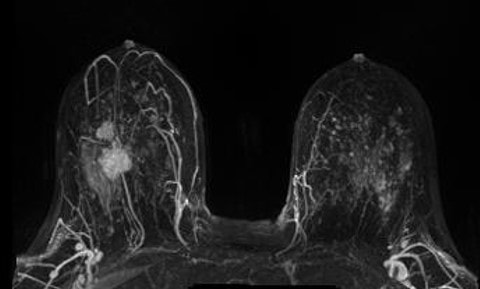
When evaluating a newly diagnosed cancer patient for extent of disease, there are a few things you want to evaluate.
|